2026-05-29
Cases of Early Revision and Correction for Double Eyelid Surgery
A detailed look at early revision for double eyelid surgery, explaining the golden time for correction (within 3 weeks) and clinical cases involving multiple folds and functional issues.
It has been a while since my last post.
Cases of Early Revision and Correction for Double Eyelid Surgery
I would like to discuss this topic today.
Early revision refers to performing surgery again when problems occur shortly after the initial double eyelid surgery, such as the appearance of multiple folds (triple folds) or when the intended crease fails to fold properly.
Generally, it is best to perform this within 2 weeks of the initial surgery, and it can be considered up to 3 weeks. While it is very rarely done within 1 month, it is not highly recommended.
This content is based on my presentation at the September 2021 Oculoplastic Surgery Research Group Symposium and recent clinical cases.
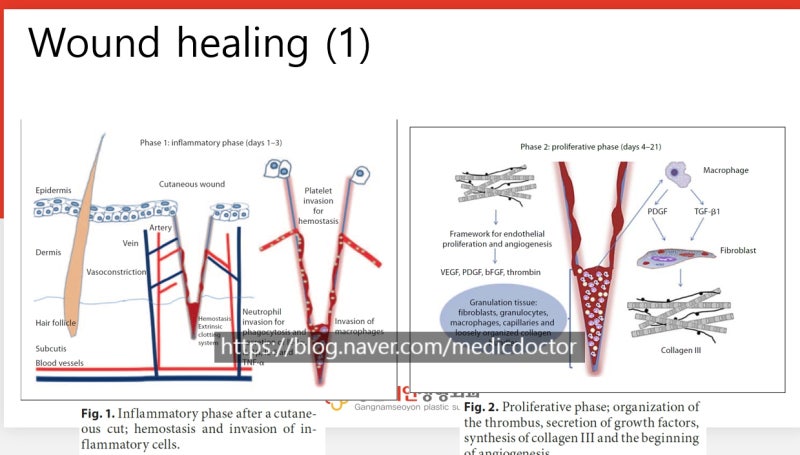
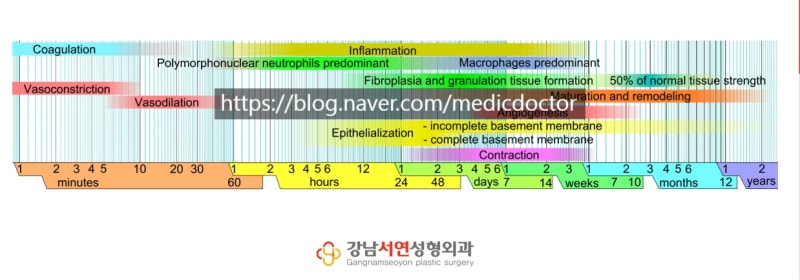
During the wound healing process, the initial ‘inflammatory phase’ involves hemostasis and the gathering of inflammatory cells to begin healing the wound.
The ‘inflammation’ mentioned here does not refer to the pus-filled infection we commonly think of, but rather the normal medical inflammatory response that occurs when a wound heals.
From day 4 to day 21, during the proliferative phase, blood clots and tissues begin to gather and knit together.
The period up to the 21st day can be considered the ‘golden time’ for early correction.
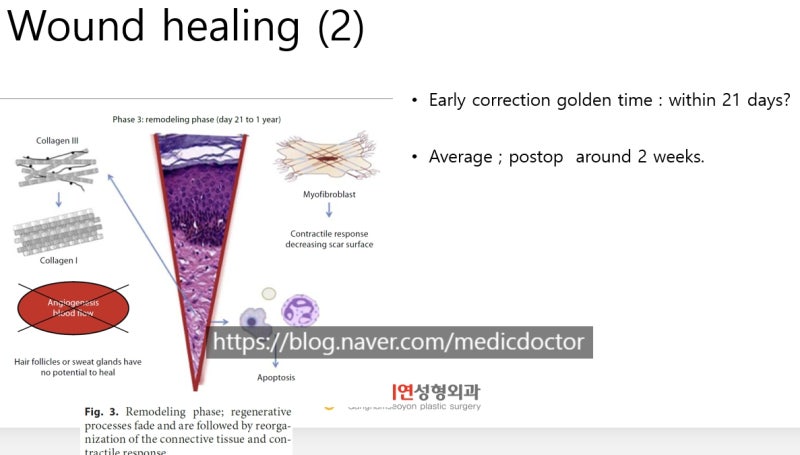
This is because the ‘remodeling phase’ (the maturation stage) begins from the 3rd week, which is when the tissues start to contract.
Generally, the period for early correction is set at up to approximately one month.
Let’s look at a recent case.
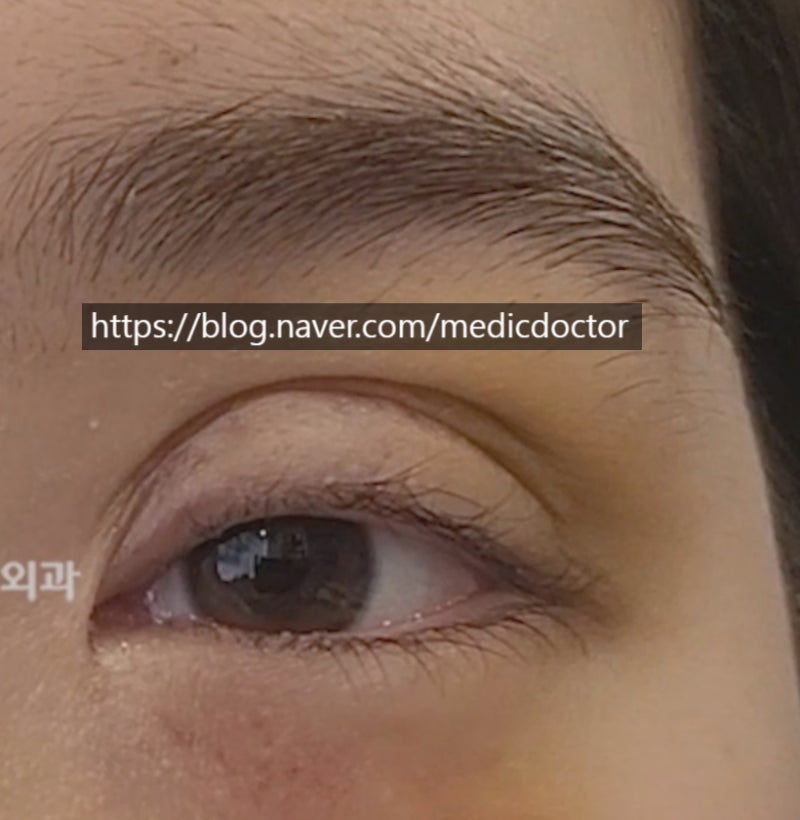
This patient had surgery at another clinic two weeks before visiting us.
They had received a follow-up correction at the previous clinic due to repeated loosening and asymmetry, but came to us complaining of multiple folds and difficulty opening their eyes.

As you can see, there are severe multiple folds on both sides, and the eyes do not open well.
There was a high probability that some form of adhesion had already occurred. Fortunately, the eyes could still open to some extent, suggesting that the levator muscle (the muscle that lifts the eyelid) was likely undamaged.
Additionally, some patients worry that fat grafting is necessary when multiple folds occur, but in this case, we successfully corrected it without any fat injection.
This is the appearance one week after the revision surgery.

The multiple folds have been resolved, and the correction was successful.
Since it has only been one week, there is still some swelling.
Looking at the patient’s pre-operative state, there is a lack of skin at the inner corner of the patient’s left eye (right side in the photo).
This specific issue cannot be fully resolved with early correction and must be addressed later after observing how the skin stretches over time.
We need to monitor the progress periodically. In the video, you can see that the multiple folds no longer appear.
However, because the previous incision line on the left (right side on video) was high at the front and more skin had been removed, the way the line folds is slightly regrettable.
This part may require further correction at the 6-month mark.
I am grateful to the patient for trusting me with their care.
Early correction usually follows this process:
It is great if everything is fixed perfectly in one go, but the reason we perform early correction is that doing it now is more advantageous than waiting. We do not perform it simply because a patient wants it.
Therefore, if waiting is the better option, it is best to wait. However, in situations like the one above, multiple folds are unlikely to improve with time, which is why early correction is performed.
First, we re-open the existing incision line.
This is because creating a new incision or cutting away more skin can make it difficult to achieve a proper correction later.
Once opened, we check for damage to the tissue itself. If there is damage, the focus is on treating that area rather than focusing solely on the aesthetic shape. This ensures a better outcome for any potential future surgeries.
For patients who cannot open their eyes properly, waiting 6 months blindly can lead to the levator muscle being severed and contracting upward, resulting in loss of function and making it extremely difficult to locate the muscle later.
Second, one must accept that the aesthetic shape can be refined again later.
When focusing on functional recovery first, slight asymmetry may occur.
During consultations, some people ask, ‘If I have to get surgery twice, why not just do it once after 6 months instead of making me go through this twice?’ This is a misunderstanding of the situation.
If a functional problem occurs, it may become unsolvable later. Perhaps because they have lost trust in other hospitals, some patients insist on waiting despite my explanations.
While it is possible for everything to be resolved at once later, I recommend early correction. It allows for a certain degree of aesthetic recovery and helps identify whether there are underlying functional issues.
I will conclude with the before and after video.
Frequently Asked Questions
When is the best time for early correction of double eyelid surgery?
It is best to do it within 2 weeks after surgery, and up to 3 weeks can be considered. From the 3rd week, the tissues in the wound area enter the maturation phase of contraction, so the period up to the 21st day is considered the golden time for early correction.
Why do early reoperations happen without waiting 6 months?
This is to solve functional problems early, such as damage to the muscles that open the eyes. If the eyes do not open well and you wait 6 months without any action, the severed muscles will contract upwards, lose their function, and become very difficult to restore later.
Does early correction involve new skin incision?
No, the existing incision line is opened. Creating a new incision line or cutting additional skin makes proper correction difficult later. Through the existing line, the extent of tissue damage is checked first.
Can early correction perfectly improve the shape?
Early correction focuses on functional recovery and treatment of tissue damage rather than shape, so some asymmetry may remain. After resolving functional problems first, it is recommended to perform a secondary re-correction for unsatisfactory cosmetic parts or line asymmetry 6 months after the surgery.
If double folds appear in the double eyelid, do I always need to inject fat?
No. Depending on the patient's condition, correction is possible without fat grafting. In actual cases, there were symptoms of double folds and difficulty opening the eyes, but successful correction was achieved by simply releasing the existing adhesions without additional fat injection.