2026-05-29
The Choice Between Double-Line and Single-Line Incisions and Examples of Early Correction
A detailed look at eyelid revision techniques, focusing on lowering high folds using double-line and single-line methods, and the importance of early correction for asymmetry.

The Choice Between Double-Line and Single-Line Incisions and Examples of Early Correction
The title sounds a bit grand, but I wanted to post this as it closely reflects my personal philosophy on plastic surgery.
First of all, ‘double-line incision’ (du-jul-tta-gi) is not a formal medical term, but since patients use this expression so frequently these days, I use it as well for familiarity.
Strictly speaking, it is a ‘double eyelid lowering’ technique that preserves the existing double eyelid scar. Please refer to my previous posts for more details.
I would like to write about a case I recently experienced.
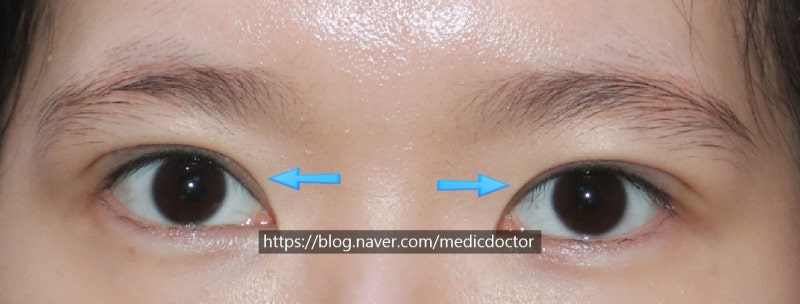
This patient has very large eyes and thin skin, but she came to me because she felt her eyelid lines were too high.
In reality, they were indeed quite high. Fortunately, her eye-opening strength was good, so the ‘sausage’ look wasn’t extremely severe, but the lines were very high and the fixation was deep (sunken scars).

The patient’s right side (left side in the photo) has a slightly higher double eyelid line.

This is the appearance when the eyes are closed. The center looks hollowed out. Because there is a lack of tissue in that area, there is a high possibility of triple folds forming after surgery.
Usually, fat grafting is performed in many cases, but personally, I am not a fan of fat grafting. However, I do perform it if absolutely necessary, though I prefer to use other methods if possible.
Surgical Plan)
1. First, plan for what is commonly called a ‘double-line incision’.

If A is the original double eyelid line, line B is designed. Aesthetically, it is best to excise the skin between A and B. While cutting it beforehand is much easier for the surgeon, there are cases where the skin appears insufficient even if it seemed redundant, due to skin condition and various other factors.
Therefore, I personally prefer to perform surgery in the safest way possible for the patient. Instead of cutting the skin in advance, I perform the double-line incision first, and then, if possible, I perform a ‘single-line incision’ by excising the old scar.
This is the appearance one week after surgery.
However, the front part of the left eyelid looks a bit low, while the front part of the right eyelid looks high.
From a surgeon’s perspective, these moments are a bit ambiguous.
I matched them perfectly right after surgery, but the right side now looks higher compared to the patient’s left eye.
In this case, I wait for one week first. I wait for the swelling to subside further. If the difference persists, I tend to perform a correction.
I asked for the patient’s understanding and requested a visit at the two-week mark.

This is the final look after removing the stitches.
Since it is only three weeks after the initial surgery, some swelling remains, but the symmetry is good, and the patient is satisfied, which makes me happy.
Since double eyelid surgery is performed by humans, slight asymmetry can occur.
While it is mostly due to swelling, if the asymmetry is clearly visible, it is usually easy to fix through early correction between 1 and 3 weeks.
However, if the doctor judges that the case will improve by waiting more than 3 months, early correction is not performed.
In this regard, you have no choice but to trust the doctor.
During consultations, I usually tell patients: ‘I don’t cut the skin in advance; I decide after opening it up,’ and ‘Please trust me.’
Revision surgery has many variables. You can predict about 80%, but the remaining 20% can only be known once you open it up.
The more surgeries I perform and the more I know, the more I find myself explaining to patients, which sometimes ends up sounding like I’m scaring them.
Even my head consultants say I seem to scare the patients too much. However, most patients will be satisfied with their surgical results.
But because I explain the potential complications that might occur in that 1% of variable cases to every patient, some might wonder, ‘Is the doctor really confident?’
However, personally, if I think it will turn out well, I recommend it; if I think it won’t, I tell them not to have the surgery.
If I recommend it, you should go ahead with the surgery.